Award-winning PDF software





Health insurance claim 1500 download Form: What You Should Know
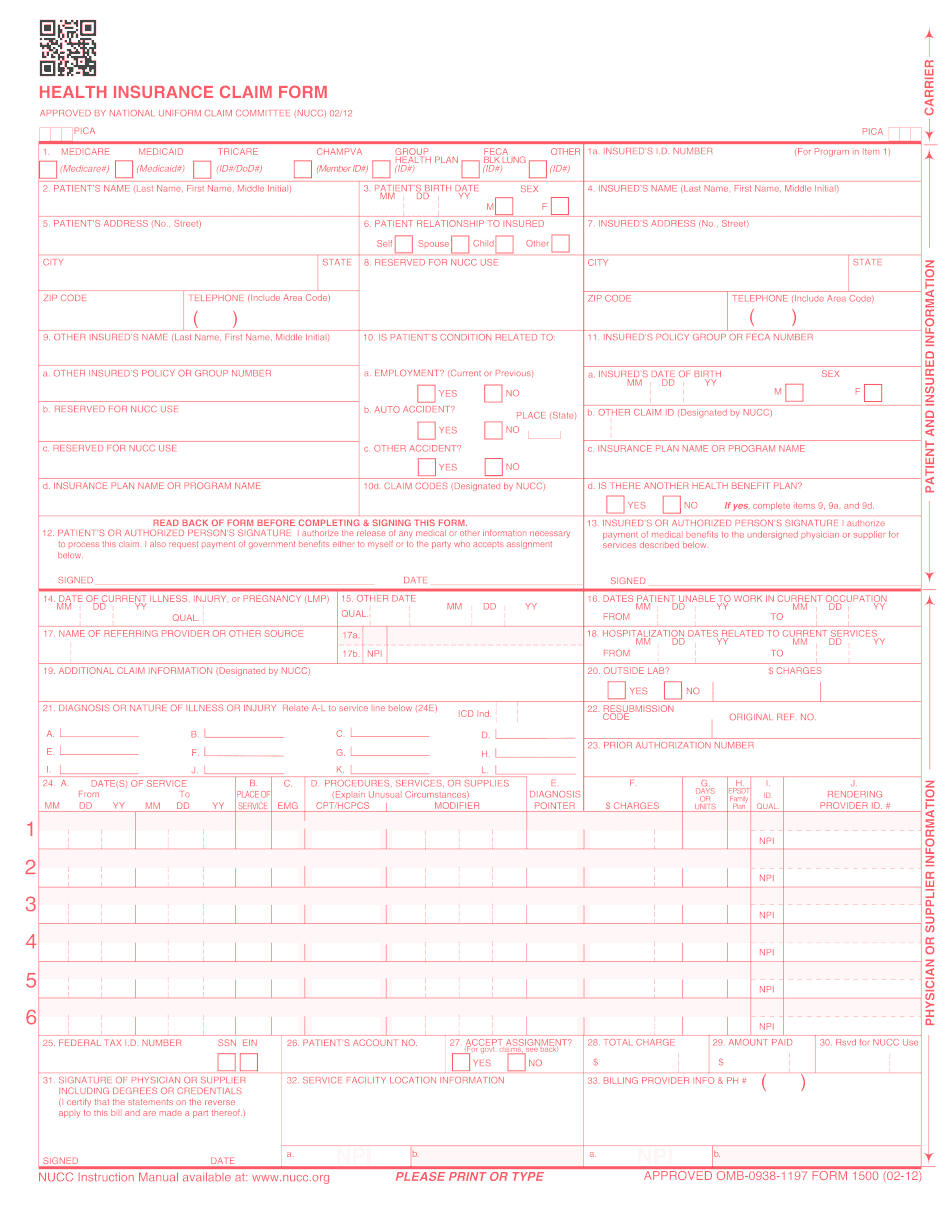
First Initial, SSN, or Date of Birth) ................................................................... 3. EMPLOYER, PARTNER'S NAME, or SHAREHOLDING MEMBER'S NAME .............................................................................. 4. EMPLOYER, PARTNER'S ADDRESS CMS1500 form — Blue Cross NC (Updated 02-12) (1) This is a paper form that requires no signature. If you require a signature, please note that you may be signed out when you submit your claim. See below for instructions. (2) All information on your claim should be completed directly on this form. However, you may provide the following additional information on the application: (a) Your age to establish your eligibility for enrollment under the plan. (b) Your marital status if filing as single or married. .................................................................. (3) The patient must answer “Yes” to all the questions. NOTE: If you are over the age of 55, and have dependent children, you must complete Part 8. If you are an employee, if you will be in attendance during your illness or injury, you may be required to answer a “Yes” on all question 11 and 12. If you are a family member eligible for disability benefits, on Question 11 you may have to answer “Yes” on Question 11(B). You do not need to answer question 11 on your own or report dependent status separately for both of your parents, if you are able. CMS1500 form — Blue Cross NC (Updated 02-12) (1) The patient must complete Part 2. (2) If there is an addendum in the attached application, add a line stating that we are requesting the medical history information on the claims associated with each medical care provider that is referred. .................................................................. (3) You may add any physician or physician's assistant to the form. This includes emergency/emergency room physicians, pain physicians, psychiatric or psychiatric assistant, physician's assistants, pharmacy, and others that have received a written authorization that allows them to sign this form. .................................................................. CMS1500 form — Blue Crosstown Medical Center (CMS-1538) — Updated 01/13. This is the CMS1500 Form 1538 for the CMS1538 Health Insurance Claim Form. A completed form must be received for your medical services provided. We will not accept a claim form for services that were not provided.
online solutions help you to manage your record administration along with raise the efficiency of the workflows. Stick to the fast guide to do Form Cms 1500 Claim, steer clear of blunders along with furnish it in a timely manner:
How to complete any Form Cms 1500 Claim online: - On the site with all the document, click on Begin immediately along with complete for the editor.
- Use your indications to submit established track record areas.
- Add your own info and speak to data.
- Make sure that you enter correct details and numbers throughout suitable areas.
- Very carefully confirm the content of the form as well as grammar along with punctuational.
- Navigate to Support area when you have questions or perhaps handle our assistance team.
- Place an electronic digital unique in your Form Cms 1500 Claim by using Sign Device.
- After the form is fully gone, media Completed.
- Deliver the particular prepared document by way of electronic mail or facsimile, art print it out or perhaps reduce the gadget.
PDF editor permits you to help make changes to your Form Cms 1500 Claim from the internet connected gadget, personalize it based on your requirements, indicator this in electronic format and also disperse differently.